Parkinson’s disease is caused by the death of one specific type of brain cell. So one researcher asked an obvious question: why not just replace them? At the time, that idea sounded impossible, as most scientists believed the adult brain could never accept new neurons. This is the story of Curt Freed, the neuroscientist who proved them wrong, performed the first fetal-cell transplants for Parkinson’s in the United States, and helped launch the entire field that stem-cell therapy now belongs to.
What goes wrong in Parkinson’s
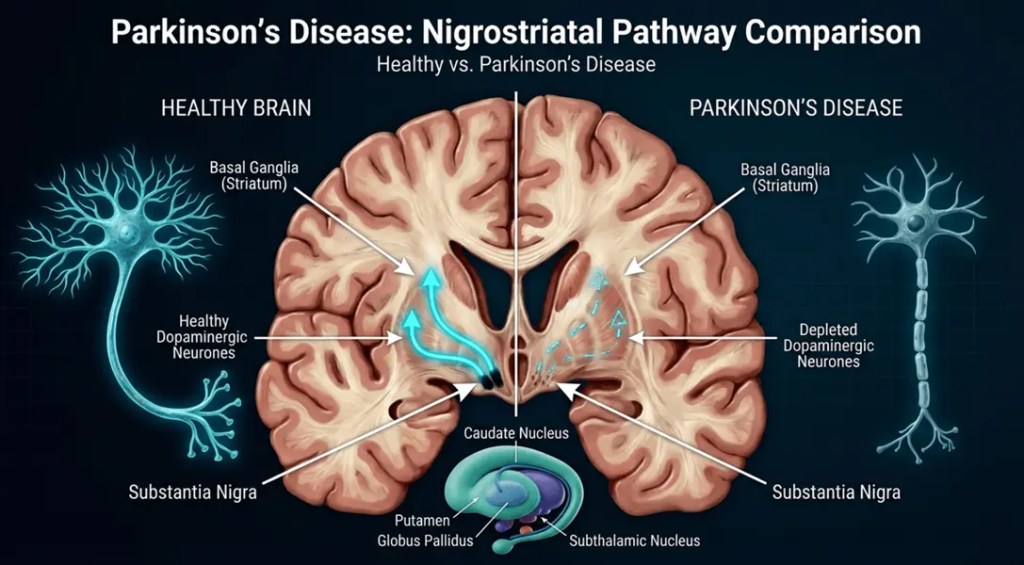
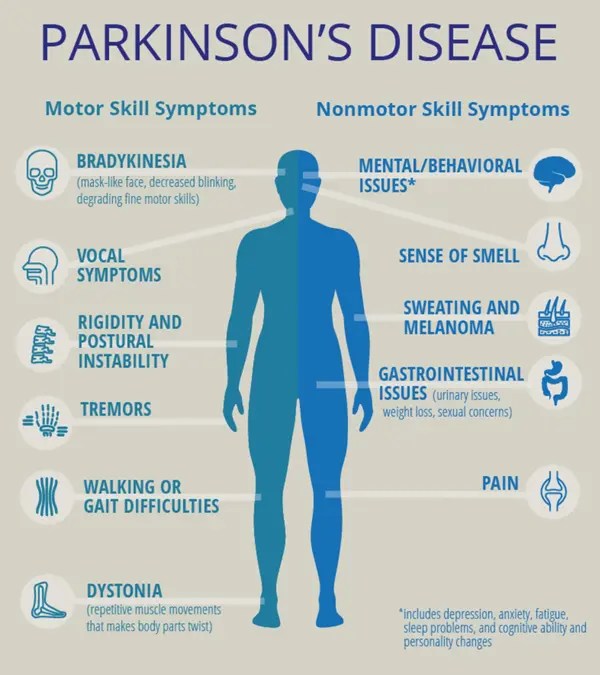
Deep in the brain is a small region called the substantia nigra. Its job is to produce dopamine, a neurotransmitter that controls movement. In Parkinson’s disease, the dopamine-producing neurons slowly die off. As they disappear, patients develop tremors, stiffness, slowed movement, and “freezing,” in which they suddenly can’t move at all.
The main treatment is a drug called L-DOPA, which the brain converts into dopamine. It works well at first, but it doesn’t stop the cells from dying. Over time, it becomes less reliable and can cause uncontrolled movements called dyskinesias.
Freed’s idea was based on a key fact: because Parkinson’s disease primarily destroys one cell type in one region of the brain, maybe you could fix it by transplanting new dopamine cells into the brain to replace the lost ones. This was a radical idea. Drugs like L-DOPA only treat symptoms; Freed wanted to actually repair the brain. Until then, brain repair was basically science fiction, and Parkinson’s was labeled “incurable.”
The evidence from animals
In the 1980s, most scientists believed the adult brain couldn’t accept new neurons. But Swedish researchers Anders Björklund and Ulf Stenevi showed that it could — if you used the right cells. When they transplanted dopamine cells derived from fetal rats into adult rat brains, the cells survived, produced dopamine, and formed connections with the host brain. Cells taken from adult rats almost always died.
The reason fetal cells survive better is that they haven’t yet developed their long fibers, tolerate low oxygen better, and are rich in chemicals that help cells grow. This became the foundation of the whole field: transplants only work with young, fetal cells.
To test whether the transplants actually helped, researchers used a rat model of Parkinson’s. They destroyed dopamine cells on one side of the brain, causing the rats to circle in a predictable direction. As transplanted cells took hold, the circling decreased. Interestingly, rats with the most new connections sometimes began circling in the opposite direction—an early sign that a transplant could overshoot and cause excessive movement. That same problem later appeared in human patients.
A new model from an accident
To move toward human treatments, scientists needed a primate model of Parkinson’s, because monkey brains are much more similar to ours. The problem was that monkeys don’t naturally develop the disease.
The solution came from a tragedy. In 1976, a college student accidentally made a chemical called MPTP while trying to produce a homemade drug. After he injected it, he developed severe Parkinson’s symptoms within days. The same chemical later poisoned several people who used a contaminated batch of street heroin in California. Researchers discovered that MPTP destroys dopamine cells in the substantia nigra. It didn’t affect rats, but in monkeys it produced a reliable form of Parkinson’s disease. Finally, scientists had an animal model close enough to humans to test transplants.
Testing transplants in monkeys
Freed’s lab at the University of Colorado was one of several groups that began transplanting fetal dopamine cells into MPTP-treated monkeys. The process involved dissecting a fetal monkey’s midbrain under a microscope, breaking the tissue into a single-cell suspension, and injecting tiny droplets into the striatum (a brain region that requires dopamine) using a precise frame to guide the needle.
The results showed both the promise and the risks. In one monkey, the transplanted side gradually improved until the animal regained a nearly normal grasp. But when the team did a second transplant on the other side, the monkey’s immune system attacked and destroyed both sets of grafted cells. The experiment taught three lessons: transplants can survive and improve symptoms, the immune system can reject them under certain conditions, and unexpected results are common at the cutting edge of medicine.
The first human patient
In November 1988, Freed and neurosurgeon Robert Breeze performed the first fetal-cell transplant for Parkinson’s in the U.S. The patient, Don Nelson, had been living with Parkinson’s for twenty years.
Because the surgery was done under local anesthetic, Nelson was awake the entire time. The team attached a metal “halo” frame to his skull, used a CT scan to map the exact target, and made ten careful passes with a needle about one millimeter wide to deliver the cells. A small piece of fetal midbrain tissue had been broken down in the lab into a cell suspension, and a dye test showed 85% of the cells were still alive before transplantation.
Mixed results and a fair test
Nelson improved over the following months. His finger movements got faster, his walking and speech improved, and he could do daily tasks he hadn’t managed in years. But he was not cured; he still moved slowly and had other symptoms. And the results across patients were inconsistent: some improved a lot, some a little, and some not at all.
Freed knew that improvement in a few patients isn’t scientific proof. Medicine has a long history of treatments that seemed to work but didn’t hold up when tested properly. So he and Stan Fahn designed a double-blind, placebo-controlled trial using sham surgery. Some patients received real transplants, while others had holes drilled in their skulls but no cells implanted. Neither the patients nor the evaluating doctors knew who got which. Every sham patient was offered a real transplant afterward.
The trial, published in 2001, found that the grafts survived in 85% of patients without immune-suppressing drugs, but only younger patients improved significantly as a group, and some patients developed dyskinesias caused by the transplant itself. The transplants worked, but adding dopamine cells alone was not a complete cure.
Why was this a turning point
It’s easy to look at the mixed results and think the work failed. It didn’t. Freed proved something that changed how scientists think about the brain: the adult human brain can accept new neurons, and replacing dead cells can actually relieve a brain disease. Before this, that was considered impossible. He showed that transplanted cells survive, produce dopamine, connect to the brain, and improve real symptoms. What’s important is that his PET scans and patient data supported it.
This established the principle of cell-replacement therapy for the brain. That principle is exactly what makes treatments for other “incurable” brain conditions like Alzheimer’s, Huntington’s, spinal cord injuries, even thinkable. Parkinson’s became the test case for the whole idea of repairing, rather than just medicating, the brain.
Freed also raised the standard for how these treatments get tested. Running a double-blind trial with sham surgery was rare and controversial, but it set an example: even dramatic-looking surgeries have to be proven against a placebo before anyone trusts them.
Why he’s a pioneer for stem-cell therapy
Here’s the key link: Freed proved that replacing lost dopamine neurons works. The problem was the source of the cells. Fetal tissue is scarce, ethically controversial, hard to standardize, and a single transplant needs tissue from several fetuses, with a risk of infection or immune rejection.
Stem cells solve every one of those problems. They can be grown in the lab in unlimited numbers, differentiated into dopamine neurons, made consistent from batch to batch, and potentially even derived from the patient’s own cells, so the immune system won’t reject them. In other words, stem cells are a far better source for the exact therapy Freed showed was possible. He was already working toward this himself, exploring lab-grown and stem-cell-derived dopamine cells before he retired.
That’s why his fetal-cell transplants are seen as the foundation of modern stem-cell therapy for Parkinson’s. He proved the concept; stem cells are now making it viable. Clinical trials today that put stem-cell-derived dopamine neurons into Parkinson’s patients are doing exactly what Freed pioneered — just with a better supply of cells.
Based on Curt Freed and Simon LeVay, Healing the Brain (2002)

Leave a comment